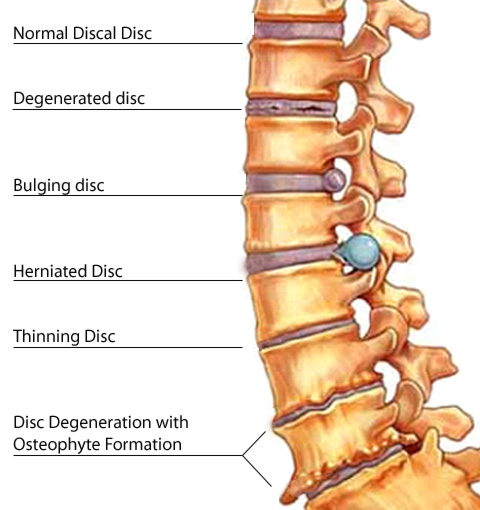
En frisk disk ska på en magnetröntgen bild ha ett ljust innehåll utan grumlighet och även ha ljusa sidor och kotorna ska inte ligga mot varandra.
Min mor har legat på sjukhus efter att hennes ben bara vek sig. Hon fick diagnosen Forestiers sjukdom med diskdegenerationer och spondolyser. Också inåt ryggmärgskanalen, en disk är nästan helt borta.
Då jag sökte efter detta ovanliga namn kom jag till Golden retrievers och veterinärmedicinska högskolan. Visst, hundar kan ha problem med ryggen.
Så hittade jag
en blogg som verkade bra. Här kommer ett stycke ur den.
Diskdegenerativ sjukdom eller DDD Diskdegeneration är en normal process som ryggraden går igenom och börjar i 45 års åldern i normala fall. På mig har det börjat extra tidigt och detta gör att jag har fått diagnosen diskdegenerativ sjukdom.
Diskdegenerativ sjukdom innebär att diskarnas innehåll ett gelé liknande vätska börjar torka och skalet, eller disk kapseln, blir skörare.Det visar sig genom att disken får svarta kanter och mörkare och ojämnare färg inuti diskarna. ( Där de blå pilarna pekar) När disk kapseln har blivit skör kan det lätt bli sprickbildningar och diskmassan rinner ut och blir diskbråck. Om diskbråcket rinner ut inåt ryggkanalen kallas det
Ritsopathi och ger ischias värk. Det är först när diskbråcket trycker på nerven i ryggkanalen som folk får ont av det och det uppstår en inflammation. Det är värk som strålar ut i ett eller båda benen. Om det blir illa nog kan man även få känselbortfall och bli delvis förlamad. I värsta fall så tappar man känsel och styrsel över underliv och rumpa. Då måste man opereras akut. 80 procent blir bättre vid en operation, 5 procent blir sämre och 15 procent får oförändrade symtom.
Det är runt 20 till 30 % av alla i Sverige som har diskbråck. Oftast känner man inte av sina diskbråck och de kan självläka men det tar över två år för dem att göra det.
En frisk disk ska vara vit vid en magnetröntgen medan en sjuk disk som har blivit degenerativ är mörkare i färgen och har stora svarta kanter. Det var i alla fall vad doktorn på Ortopeden i Umeå sa till mig.
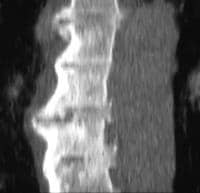
Den övre disken på bild nummer två har svarta fällt i sig och är väldigt sjuk, även det med diskbråcket i är en väldigt sjuk disk. Där diskbråcket är har det även blivit kalk ovanför så diskbråcket rinner ut nedanför kalkavlagringen. Det innebär att jag antagligen har haft det diskbråcket väldigt länge. För när man har haft diskbråck och det ska "läka" så bildar kroppen ett kalklager för att kapsla in disken.
Mitt diskbråck rinner därför ut under detta kalklager och mina "mycket trasiga och sjuka diskar" ser ut som på bilderna ovan.

Diskdegenerationen är det svarta till vänster i disken.
Blå pilar: Är diskdegeneration i diskarna.
Svart pil och Svart Text är ryggkanalen där nerver och ryggmärgsvätskan håller till
Den Lila Pilen är på Nerven
Den röda pilen och texten är Kalkavlagring som finns på ett diskbråck.
den mörkblå pilen är ett diskbråck som rinner ut under kalkavlagringen.
Så hittar jag nåt som passar på
netdoktorn. Verkar vara som jag gissade, Bechterevs sjukdom har spaltats upp? Min mor har
diagnosen Bechterev (nyttig information) från tidigare. Hon har också gikt som spökat igen nu på sistone. Båda hör till reumatiska gruppen.
Fråga: Är en kvinna på 48 år som fått diagnos Morbus Forestier, har sökt information runt den sjukdomen men hittar inget på svenska...

Esbjörn Larsson
överläkare, Reumatologkliniken, Karolinska Universitetssjukhuset, Solna svarar:
Morbus Forestier kallas även för DISH ( diffus idiopatisk skeletal hyperostos) och innebär förkalkning av ligament kring ryggraden men även bennybildningar kring leder på andra ställen i kroppen. Orsaken är okänd detta kan ge stelhet men många gånger upptäcks detta tillstånd vid röntgen av ryggen aven slump då man letar andra sjukdomar. Symtomen kan variera från inga symtom alls till mycket besvär i form av smärta och stelhet från rygg och leder och om halsryggen är drabbad har sväljningssvårigheter beskrivits. Då orsaken är okänd finns tyvärr ingen bot. Sjukgymnastisk träning lindrar ofta symtomen och ibland måste smärtstillande läkemedel användas. När det gäller arbetsförmåga måste varje patient bedömas efter hur det påverkar arbetsförmågan . Mer information kan hittas på internet och pröva att gå in på www.ki.se och välj bibliotek Så en svensk
Cutting Edge tidning för läkare: Peter Croft från Storbritannien talade om forskning om muskuloskeletal smärta.
Han inledde med några allmänna konstateranden som han själv beskrev som ”certainly not cutting edge”:
– Smärta är vanligt förekommande bland befolkningen, och den vanligaste smärtan är muskuloskeletal. Enligt våra prognoser kommer det att bli ett ännu vanligare tillstånd i framtiden. Med data från brittisk primärvård kunde Peter visa att just ryggsmärtor var det allra vanligaste som man sökte läkarvård för. 45% av de vuxna som sökt hjälp, hade kvar samma smärta 14 månader efter första läkarbesöket.
–
Att jaga efter en diagnos verkar alltså inte hjälpa särskilt mycket, konstaterade han.
Så vad kan man då göra istället? Ett försök att förändra modellen genom att tackla andra omständigheter runt smärtpatienten genom en psykologisk approach, har i en studie inte visat sig ge något bättre resultat.
Därför måste man förändra fokus: Från att söka efter en diagnos och orsaker, tillatt istället inrikta sig på att behandla de problem som uppstår av smärta och de funktionsstörningar den ger upphov till.– Vi måste försöka identifiera våra mål med vår behandling, strukturera dem ochgradera dem inbördes. Skilja på begrepp som försämring och funktionell begränsning, samt restriktioner att utföra en viss handling. Kan patienten deltaga i de olika aspekter av livet som patienten vill? Det kan t.ex. handla om att lyfta en resväska eller spela golf.
Det låter ju som alternativ terapi. Det är den dysfunktionella situationen som måste lösas.
InflammasomenAlexander So, från Schweiz, talade om hyperurikemi och gikt.
Alexander redogjorde för begreppet
inflammasom som blev myntat för några år sedan. Det är en samling proteiner som styr cellernas produktion av interleukin-1 (IL 1).
Vid gikt triggar uratkristallerna i blodet en inflammatorisk kaskad genom att aktivera inflammasomen. IL-1-blockerare verkar hämma denna inflammatoriska process. Renala transportproteiner för urinsyra har också blivit identifierade, och därför representerar även dessa lämpliga mål får framtida terapier.
Aggrecan.
Den föreläsare som rest allra längst väg var Amanda J Fosang som kom från Australien. Hon talade om
aggrecan, som tillsammans med Typ-2 kollagen, utgör en strukturellt viktig komponent för brosk. Hon berättade om försök på möss där hennes forskargrupp inaktiverat gener för kollagenas- och aggrecanasaktivitet, för att se om detta innebar en möjlighet att skydda ledbrosk från nedbrytning.
Tidningen innehöll också en notis:
Forestier, Jaques (1890–1978), fransk reumatolog som under sin aktiva tid efterträdde sin far Henri som chef för behandlingscentret Aix-les-Baines.
Han beskrev 1950 tillsammans med spanjoren Jaime Rotes-Querol ett syndrom de kallade ”senile ankylosing hyperostostosis of the spine”. Detta kallas numera diffus idiopatisk skeletal hyperostos (DISH) eller Forestier-Rotes-Querols sjukdom.
Forestier J, Rotes-Querol J. Senile ankylosing hyperostosis of the spine. Ann rheum Dis 1950;9: 321-30.Leden I. Jacques Forestier. Grundaren av fransk reumatologi. ReumaBulletinen (nr 64) 2006: 20-21.Vilka är målen för vår rehabiliterande verksamhet?Enligt Socialstyrelsens definition är rehabilitering insatser som skall bidra till att en person med funktionsnedsättning ”utifrån dennes behov och förutsättningar, återvinner eller bibehåller bästa möjliga funktionsförmåga samt skapar goda villkor för ett självständigt liv och ett aktivt deltagande i samhällslivet” (SOSFS 2008:20). Karakteristiskt för rehabilitering är att flera
åtgärder samordnas och att många professioner är aktiva.
WHO presenterade 2001 en internationell klassifikation och biopsykosocial modell kallad ”International Classification of Functioning, Disability and Health, ICF”. Functionshinder, funktionshinder, functionshinder...
Enligt ICF kan komponenterna i ett funktionshinder relateras till en hälsobetingelse, exempelvis RA.
HälsobetingelseStörning/sjukdomExempel RA
Kroppsfunktion ochanatomisk strukturFunktionshinder:
Funktionsnedsättning
Strukturavvikelse
(smärta, nedsatt rörlighet)
AktivitetFunktionshinder:
Aktivitetsbegränsning
(svårt att klara
personlig vård)
DelaktighetFunktionshinder:
Delaktighetsinskränkning
(ej delaktig i yrkesliv)
Omgivningsfaktorer
Barriärer hinder
(produkter, teknik,
omgivningens attityder)
Personliga faktorer
Ej klassificerade
(ålder, kön, livsstil,
utbildning, coping nämns)
emedicine har en bättre artikel, men på engelska.
Pathophysiology
Diffuse idiopathic skeletal hyperostosis (DISH) is characterized by a tendency toward ossification of ligament, tendon, and joint capsule (enthesial) insertions.[13] DISH is a completely asymptomatic phenomenon; no alterations are detectable based on history or through physical examination.
Epidemiology Frequency United States
Diffuse idiopathic skeletal hyperostosis (DISH) is present in approximately 19% of men and 4% of women older than 50 years. Frequency information in the US was derived from the study of nonselected skeletal/cemetery populations.[14]
International
The posterior longitudinal ligament of the cervical spine is ossified in 2% of Japanese individuals but in only 0.16% of white persons.[15] The anterior longitudinal ligament is calcified in 24% of patients with posterior longitudinal ligament ossification.[16] Diffuse idiopathic skeletal hyperostosis (DISH) was reported in 17% of individuals in the Netherlands, paradoxically with male predominance.[17]
Mortality/Morbidity
Diffuse idiopathic skeletal hyperostosis (DISH) appears to be a phenomenon rather than a disease. Double-blind controlled evaluation (in which controls and patients were drawn from the same population) revealed no associated pathology. Arthritis, bursitis, and tendinitis appeared no more frequently in patients with DISH than in controls. Any back pain present was no different in character or duration than that noted in control subjects. A history of back injury was actually found to be twice as frequent in control subjects as it was in patients with DISH. Back flexibility was no more limited in patients with DISH than it was in controls. In fact, patients with DISH who had decreased lumbar spinal motion had a lower frequency of back pain, implying that DISH may be protective.[14, 18] One study has showed that DISH may be protective against back pain.[19]
Race
The posterior longitudinal ligament of the cervical spine is ossified in 2% of Japanese individuals but in only 0.16% of whites.
Sex
Diffuse idiopathic skeletal hyperostosis (DISH) is present in approximately 19% of men older than 50 years but is found in only 4% of women in this age group.
Age
Diffuse idiopathic skeletal hyperostosis (DISH) is uncommon in patients younger than 50 years and is extremely rare in patients younger than 40 years.
A study from Finland
[20] revealed the age frequency in Finnish men to be as follows:
- 40-49 years - 0.3%
- 50-59 years - 2.7%
- 60-69 years - 8.4%
- 70 years or older - 11.2%
The same study revealed the age frequency in Finnish women to be as follows:
- 40-49 years - 0.2%
- 50-59 years - 1.7%
- 60-69 years - 4.3%
- 70 years or older - 6.9%
History
Diffuse idiopathic skeletal hyperostosis (DISH) is an asymptomatic phenomenon. The condition is discovered inadvertently. Rarely, dysphagia may result, either from neuropathy or from physical impingement by bony overgrowth.
Physical
If vertebral fusion is quite extensive, reduction in range of spinal motion occurs.[21] Because uniform vertebral involvement is extremely rare, no relatable findings exist.
Causes
Causes are unknown. Diffuse idiopathic skeletal hyperostosis (DISH) is simply a tendency toward calcification of entheses.
Differentials
Overview
Paraspinal ligaments undergo degeneration secondary to attrition, and they often ossify, a condition broadly termed spinal enthesopathy. Physicians recognize Forestier disease (involves the anterior longitudinal ligament), diffuse idiopathic skeletal hyperostosis (DISH) (more diffuse variant of Forestier disease which exhibits additional extra-axial features), and ossification of the posterior longitudinal ligament (OPLL) as being associated with this phenomenon.
Clinically, DISH is often referred to as senile ankylosing spondylitis, because there are similarities in appearance between the 2 conditions; however, DISH and ankylosing spondylitis differ in their age of onset. See the following images.
 Radiograph of the lumbosacral spine (anteroposterior view) showing flowing osteophytes and soft-tissue ligamentous ossification consistent with diffuse idiopathic skeletal hyperostosis.
Radiograph of the lumbosacral spine (anteroposterior view) showing flowing osteophytes and soft-tissue ligamentous ossification consistent with diffuse idiopathic skeletal hyperostosis.  Sagittal, T2-weighted magnetic resonance image of the cervical spine showing ossification of the posterior longitudinal ligament. Courtesy of A. Vincent Thamburaj, MD, Apollo Hospital, Chennai, India.
Sagittal, T2-weighted magnetic resonance image of the cervical spine showing ossification of the posterior longitudinal ligament. Courtesy of A. Vincent Thamburaj, MD, Apollo Hospital, Chennai, India. DISH diagnostic criteria
The following features are used to diagnose DISH[1] :
Flowing calcifications and ossifications along the anterolateral aspect of at least 4 contiguous vertebral bodies, with or without osteophytes
Preservation of disk height in the involved areas and an absence of excessive disk disease
Absence of bony ankylosis of facet joints and absence of sacroiliac erosion, sclerosis, or bony fusion, although narrowing and sclerosis of facet joints are acceptable
[2]
Unlike ankylosing spondylitis, DISH does not involve the sacroiliac joint. DISH is also distinct from marginal osteophytes that form in response to degenerative disk disease. Patients with DISH infrequently demonstrate disk height reduction or vacuum changes.
Lower thoracic spine involvement is typical of DISH, but the lumbar and cervical spine can also be affected. The left side of the spine is typically spared or less involved, which is probably attributable to the pulsating aorta. Forestier disease includes many extra-axial features, such as ossification of other ligaments and tendons, as well as subcutaneous calcification.
Preferred examination
Radiography of the thoracic and lumbar spine usually is sufficient for diagnosing DISH. Occasionally, computed tomography (CT) scanning may be performed to evaluate complications, such as fracture, or symptoms caused by pressure effects on the trachea, esophagus, and veins. Bone scanning and magnetic resonance imaging (MRI) do not play a significant role in the diagnosis of DISH.
Limitations of techniques
Radiography of the spine is the single most useful imaging modality in the diagnosis of DISH. However, patient body habitus or an inability of the patient to lie on his or her side for a lateral view may compromise the quality of radiographs. In addition, radiographs are inadequate for evaluating the extent of the compression caused by the large syndesmophytes on the trachea, bronchi, or esophagus. In this case, CT scanning of the spine is helpful and especially is aided by coronal and sagittal reconstructions.
Conversely, CT scanning usually is not cost-effective for imaging the entire spine and provides limited information about spinal cord involvement. In this situation, MRI is of benefit and thus is reserved primarily for evaluating possible cord compression. This is especially true if DISH is associated with OPLL, as it is in a minority of patients.[1]
Differential diagnosis and other problems to be considered
The differential diagnosis includes ankylosing spondylitis, neuropathic arthropathy (Charcot joint), primary osteoarthritis, and psoriatic arthritis. Musculoskeletal involvement in Reiter syndrome is another condition to be considered.
Radiography
Radiographs of the spine in patients with diffuse idiopathic skeletal hyperostosis (DISH) typically demonstrate thoracic spinal involvement; however, this condition can also affect the lumbar and cervical spine. DISH is distinguished by the presence of flowing syndesmophytes along, but separated from, the anterior aspect of the vertebral bodies, involving at least 4 levels. The disease begins as fine ossification, 1- to 2-mm thick, but ossification may thicken to as much as 20 mm as the disease progresses.
Extra-axial radiographic findings in DISH include ossification of the nuchal ligaments of the skull; enthesopathy at the ischial tuberosities in the pelvis, as well as ossification of the sacrotuberous ligament and the symphysis pubis; ossification of the triceps tendon in the upper extremities, and subcutaneous calcification of the skin.
The following radiographs show DISH.
Radiograph of the lumbosacral spine (anteroposterior view) showing flowing osteophytes and soft-tissue ligamentous ossification consistent with diffuse idiopathic skeletal hyperostosis.  Radiograph of the lumbosacral spine (lateral view) showing flowing anterior osteophytes indicative of diffuse idiopathic skeletal hyperostosis.
Radiograph of the lumbosacral spine (lateral view) showing flowing anterior osteophytes indicative of diffuse idiopathic skeletal hyperostosis.  Radiograph of the thoracic spine (anteroposterior view) showing osteophytes on the right side only, a feature typical of diffuse idiopathic skeletal hyperostosis.
Radiograph of the thoracic spine (anteroposterior view) showing osteophytes on the right side only, a feature typical of diffuse idiopathic skeletal hyperostosis. Degree of confidence
The hallmark of DISH is ossification occurring along the anterior aspect of the vertebral bodies but remaining separate from the vertebrae. Osteophytes of degenerative spinal disease usually occur along the anterolateral aspect. The location of the ossification distinguishes DISH from ossification of the posterior longitudinal ligament (OPLL).[3]
False positives/negatives
Omnipresent degenerative osteophytes represent the most common finding that mimics DISH; however, DISH is defined by the strict criteria of anterior location and the bridging involvement of 4 contiguous vertebral bodies (3 intervertebral disk spaces).
Computed Tomography
CT scanning is usually not indicated in diffuse idiopathic skeletal hyperostosis (DISH), unless there is a need to evaluate complications, such as fracture, spinal canal stenosis secondary to associated ossification of the posterior longitudinal ligament (OPLL), and pressure effects on the esophagus or inferior vena cava.
CT scans show ossification along the anterior aspect (see the following image), and coronal reconstruction depicts the classic pattern.
 Lateral reconstruction computed tomography (CT) scan showing anterior syndesmophytes.
Lateral reconstruction computed tomography (CT) scan showing anterior syndesmophytes. 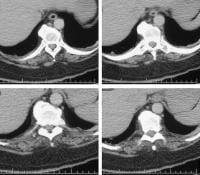 Computed tomography (CT) scans showing large, flowing syndesmophytes.
Computed tomography (CT) scans showing large, flowing syndesmophytes. Degree of confidence
The same criteria used in radiographic evaluation (the location of the ossification and an involvement over at least 4 vertebral bodies) define DISH and distinguish this entity from degenerative osteophytes.
Magnetic Resonance Imaging
MRI of the spine is usually not indicated in diffuse idiopathic skeletal hyperostosis (DISH), because the diagnosis is made using plain radiographic findings. CT scanning, using coronal and sagittal reconstruction, is useful because it provides better anatomic definition.
When associated ossification of the posterior longitudinal ligament (OPLL) causes neurologic symptoms, MRI is valuable for determining the extent of the ossification, the mass effect on the thecal sac, and the presence of cord compression. Typically, DISH manifests as a long segment of low T1 and T2 signals that is anterior to several contiguous vertebrae, whereas OPLL manifests as a signal that is posterior to the vertebral body and that extends for several segments. Cord edema manifests as a high T2 signal. See the image below.
Sagittal, T2-weighted magnetic resonance image of the cervical spine showing ossification of the posterior longitudinal ligament. Courtesy of A. Vincent Thamburaj, MD, Apollo Hospital, Chennai, India.
Nuclear Imaging
In nuclear medicine, bone scanning is usually requested for the evaluation of back pain, revealing the nonspecific pattern of the diffusely increased and heterogeneous uptake of radiopharmaceutical agents in the spine (see the image below). Diagnosis relies primarily on the use of radiographs.
 Bone scan showing heterogeneous, nonspecific increased uptake in the spine with 2 additional focal hotspots.
Bone scan showing heterogeneous, nonspecific increased uptake in the spine with 2 additional focal hotspots. Degree of confidence
The appearance of diffuse idiopathic skeletal hyperostosis (DISH) on a bone scan is nonspecific, and without radiographic correlation, diagnosis is difficult.